Gastric cancer is an aggressive malignancy that can sometimes be cured with surgery. The details of surgical resection have led to a relatively complicated nomenclature regarding the extent of lymph node removal. This lesson will explain the terminology.
The stomach is situated in the abdomen just below the diaphragm. The esophagus feeds into the stomach proximally, and the stomach empties into the duodenum. These structures are easier to see when the diaphragm is removed.
The major vascular supply to the stomach is through various gastric arteries which arise from the celiac trunk or the splenic artery. The arteries can be viewed from the posterior aspect with the stomach in situ. Other important vascular structures include the hepatic artery and the aorta.
Lymph nodes tend to follow the arterial structures. As mentioned above, surgery is potentially curative in patients with gastric cancer. The extent of surgery is somewhat controversial, particularly regarding the removal of lymph nodes.
Terminology has developed to include terms such as D1, D2, D3 and even D4 nodal resections. These terms are meant to describe the dissection of nodal groups N1-N4. Variations in the extent of resection have been termed D1+, D2-, etc. These terms are based on the local, regional, and distant lymph node chains which surround the stomach.
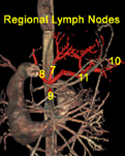
The figures at the right show (from top to bottom): A map of the perigastric (N1) nodal groups, the regional (N2) nodal groups, and the distant (N3,N4) nodal groups.
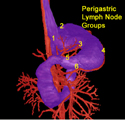

In general, a wide margin of resection is performed on the primary tumor in the stomach, including removal of the omentum. A D1 resection also removes nodes directly adjacent to the stomach. The particular nodal sites included in a D1 resection depend on the tumor location in the stomach. For instance, a proximal gastric tumor would include nodal groups 1-4, whereas a distal gastric tumor would include groups 3-6. (See top figure for location of the specific nodal sites.)
Japanese surgeons routinely perform extended lymphadenectomy, or D2 resections, with removal of perigastric nodes and nodes along the left gastric, common hepatic, celiac and splenic arteries. These arteries can be identified by moving the mouse cursor over the dissection image. Previously, a D2 resection also included removal of the spleen and part of the pancreas, but now these organs are preserved through meticulous technique. Again, the nodes included in a D2 resection vary somewhat with the location of the tumor. A proximal gastric tumor surgery would include nodal groups 1-4 plus 5-11 in a D2 resection, whereas a distal gastric cancer surgery would include nodal groups 3-6 plus 1, 7-9 in a D2 resection. (See the top two figures for locations of the specific nodal sites.)
More aggressive D3 surgery includes removal of nodes along the hilum of the liver, behind the pancreas and under the transverse colon. In a D3 resection, a proximal gastric tumor surgery would be removed with nodes 1-4 plus 5-11 plus 12-14. A distal gastric cancer resection would include nodal groups 3-6 plus 1, 7-9 plus 2, 10-14. (See figures for the location of the specific nodal sites.)
Recently, a more aggressive surgery, the D4 resection has been developed which removes nodes along the aorta from the diaphragm hiatus to the iliac bifurcation.
Following surgery, the UICC's classification of residual tumors (R) after the operation include complete resection (R0), microscopic residual tumor (R1) and macroscopic residual tumor (R2). Depending on the surgery terms such as R0D2 can be used which imply a complete resection of all tumors through a D2 gastrectomy.
A general rule is that the more extensive the surgery, the more morbid the procedure. In Japanese series, it appears that more aggressive D2 resection, and possibly even D3/ D4 surgeries may provide a survival advantage. However, in a large randomized European series (the Dutch Gastric Cancer Trial), there appeared to be no survival difference in those who underwent a more morbid D2 surgery compared to a limited (D1) lymph node dissection, and in general, Western surgeons perform a D1, or D1+ surgery.