Some cases of shoulder pain arise outside of the shoulder structures from remote visceral organs or adjacent musculoskeletal structures. Well-localized shoulder pain usually arises from shoulder joint structures and is transmitted via branches of the Brachial Plexus innervating these structures. Extrinsic causes of referred shoulder pain arise from:
- Pain from Disease in the Neck
- Pain from Neuromuscular Structures
- Suspensory Muscular Pain
- Pain from Distant Viscera
Cervical spine arthritis and degenerative disk disease describe posterior neck-shoulder pain that is affected by movement of the neck rather than movement of the shoulder. Patients usually have paracervical muscle spasm and tenderness to deep palpation. Neck range of motion is decreased and pain is increased with flexion, extension, rotation and lateral bending of the cervical spine.
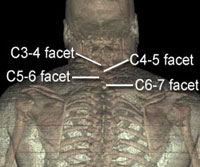
Facet joint pain with cervical spondylosis produces radiating pain without a neurologic deficit. Pain is not increased by shoulder motion but by neck motion. Shoulder motion is normal but neck motion is limited.
- C3-4 Facet pain: Pain in suboccipital region and posterolateral neck/medial aspect of the top of the shoulder
- C4-5 Facet pain: Pain in base of the neck reaching out over the medial aspect of the posterior shoulder
- C5-6 Facet pain: Pain is felt in the shoulder region out over the Deltoid and into the interscapular region
- C6-7 facet pain: Pain is felt in the Supraspinatus and Infraspinatus fossae
Shoulder plus radiating arm pain is caused by spinal cord tumors, herniated disk, foraminal root compression, scalene and cervical rib syndromes and clavipectoral compression syndromes. These pains go below the elbow and into the hand and fingers with a sharp tingling character and a darting or lancinating quality. It is often intermittent and may be associated with numbness and sensory changes on examination. Persistent shoulder pain with motor and sensory changes without a history of trauma should prompt evaluation for a cervical spine tumor.
Compression and/or irritation of cervical roots is due to herniated disk, foraminal stenosis, tumor, osteophyte, or (rarely) infection. Associated neurologic symptoms may include numbness, tingling, paresthesias, weakness and loss of reflexes. MRI is the best test to illustrate anatomical abnormalities and electromyogram with nerve conduction studies will provide neurophysiologic assessment of each nerve root. Each root has a characteristic dermatome pain pattern and pattern of neurologic deficits. The pain is initiated or exacerbated by neck motions rather than shoulder movement. The Spurling test, combination of neck extension and head tilt toward the affected side with pressure exerted downward on the patient's head may reproduce the pain pattern.
- C5 Root: Pain in neck, shoulder, anterolateral arm with numbness in Deltoid area, weakness in Deltoid and Biceps muscles and decrease in Biceps reflex.
- C6 Root: Pain in neck, shoulder, lateral arm with numbness in dorsolateral aspect of thumb and index finger, weakness of Biceps, wrist extensors and Pollicis Longus with decrease in Brachioradialis reflex.
- C7 Root: Pain in neck shoulder, lateral arm and dorsal forearm with numbness in index and middle finger and dorsum of the hand, weakness of Triceps and decrease in Triceps reflex.
Produces deep severe pain from the Supraclavicular area into the arm and is usually associated with weakness. The pain is described as a deep, boring pain exacerbated by movement of the neck and shoulder. Patients should undergo MRI of the neck and shoulder region and electromyography with nerve conduction studies to localize the pathology. The plexopathy is produced by:
- Compression of the plexus by the first rib or muscles (Thoracic Outlet Syndrome)
- Tumor invasion (Pancoast syndrome with Horner's sign)
- Direct trauma and stretch injuries
- Irradiation injury
- Inflammatory causes (Parsonage-Turner syndrome) produces acute severe pain that is burning and involves the shoulder and upper lateral arm and is unaffected by neck motion. The pain is often more severe at night and is rapidly accompanied by muscle weakness and atrophy.
Suprascapular Nerve entrapment causes compression of the Suprascapular Nerve at the Suprascapular Notch. This commonly occurs with wearing backpacks or direct blows to the shoulder in sports and with falls that cause a nerve stretch injury. The Suprascapular Nerve (C5, C6) innervates the Supraspinatus and Infraspinatus muscles and is the sensory nerve to the Glenohumeral Capsule and the Acromioclavicular Joint. Compression or injury to the nerve causes a severe deep burning and/or aching pain from the top of the Scapula out over the postero-lateral shoulder. There is tenderness to palpation of the Suprascapular Notch and weakness of the Supraspinatus (abduction) and Infraspinatus muscles (external rotation) with atrophy. The pain can be exacerbated by reaching across the chest and rotating the neck away from the painful shoulder.

The neurovascular bundle of the Subclavian Artery and vein with the Brachial Plexus may be compressed between the Scalene muscles and the first rib at the Thoracic Outlet.
This compression produces a constellation of symptoms - pain, paresthesiae and numbness from the antero-superior aspect of the shoulder down the arm and into digits 4 and 5 that may be exacerbated by activities. Associated symptoms related to vascular irritation include discoloration, temperature change, arm claudication, and Raynaud's phenomenon. This compression may be caused by a cervical rib, elongated C7 transverse process, fracture or exostoses.



Posterior Neck/Shoulder discomfort or aching may be due to a variety of abnormalities in the suspensory muscles. Mechanical stretch due to abnormal posture or muscle weakness from paralytic neurologic disorders produces pain that is not initiated or exacerbated by shoulder motion.
Weakness in suspensory muscles may be caused by:
- Spinal accessory nerve paralysis causes Trapezius paralysis following shoulder injury or cervical node biopsy. There is drooping of the shoulder with a dragging, aching pain and attempts at abduction increase the pain.
- Long thoracic nerve paralysis (C5.C6,C7 ) causes Serratus Anterior palsy
- Axillary Nerve injury from trauma to the back of the shoulder, Humerus fractures, during surgery (Deltoid and Teres Minor weakness ).
- Fracture or tumor in cervical vertebrae characteristically cause a constant deep boring neck to shoulder pain that may be severely exacerbated by neck motion and may be accompanied by systemic features of malignancy.
Mechanisms causing shoulder pain referred from remote viscera are poorly understood. Nociceptive impulses from the Diaphram via the Phrenic Nerve produce pain in the Trapezius, Supraclavicular area and Superior Angle of the Scapula. Cardiac pain is referred to the Axilla, Left Pectoral region. Pain in the inner arm and anterior neck is associated with exertion. Gallbladder irritation refers pain to the tip of the shoulder and Scapular region. The Phrenic Nerve may also be irritated by lesions in the upper thorax (Pulmonary Sulcus Tumor with Pancoast's Syndrome), Pleura, Mediastinum and Pericardium. It is important to note that referred pain may also be associated with cutaneous hypersensitivity and muscle spasm.