by Adam Lawson BA, MSc and Terra Doucette Hiller BA, BSN, RN
Conduction System of the Heart
The conductive tissues of the heart transmit electrical signals in a hierarchical fashion. For each heart beat, the signals originate in the sinu-atrial node and terminate in the ventricular myocardium.
Sinu-atrial node (a.k.a., sinoatrial node, SA node) - generates the initial electrical signals of sinus rhythm.
both the left and right coronary arteries (~5% cases)
It rhythmically initiates impulses around 60-100 beats per minute (BPM).
Electrical conduction from the SA node travels through the myocardium of the atrium causing the right and left atrium and the interatrial septum to contract simultaneously and depolarize.
Atrioventricular node (a.k.a., AV node) - conducts electrical signals from the depolarized atria to the ventricular nerve fibers.
It delays conduction to allow time for ventricular filling and to receive all action potentials arriving from the atria.
Bundle of His - conducts electrical signals from the AV node to the bundle branches.
It runs through the intraventricular septum and divides into a right and left bundle branch.
Bundle Branches
Right bundle branch - runs along the right side of the septum to the heart apex and carries the impulse to the right ventricle.
Left bundle branch - runs along the left side of the septum to the heart apex and carries the impulse to the left ventricle.
Purkinje fibers - conduct electrical signals from the bundle branches to the ventricular muscle.
Purkinje fibers arise from contributions of the right bundle branch and the anterior and median fascicle of the anterior bundle branch.
The purkinje fibers divide multiple times before terminating in the myocardial cells themselves in the ventricles.
The fastest conduction velocity of all the heart tissue happens in the purkinje fibers, which contributes to the depolarization of the ventricular muscle.
Nervous Control of the Heart Rate
Extrinsic hormones and neurons can influence the heart rate.
Nerve fibers branching from the spinal cord at the level of T1-L2 vertebrae primarily innervate and influence the ventricular contraction rate.
The sympathetic fibers release norepinephrine which increases the rate of nodal depolarization and strengthens myocardial contractility (i.e., a positive inotropic effect).
Other sympathetic control comes from the release of norepinephrine and epinephrine into the bloodstream from the adrenal medulla.
Cardiopulmonary Receptors
Specialized cells at various locations in the body provide feedback that influences cardiopulmonary function.
Baroreceptors (pressure receptors) - monitor arterial pressure and arterial wall conformation and signal the nervous system to responsively raise or lower blood pressure, breathing rate, and heart rate.
In the Bainbridge reflex (a.k.a., the atrial reflex):
Right atrial receptors monitor stretch of the right atrial wall resulting from increase in venous return.
Overstretching of the atrial wall signals the medulla.
Medullary control centers send signals that equalize pressures in the heart by inducing tachycardia.
Electrocardiogram
An electrocardiogram (a.k.a., ECG, EKG) monitors the electrical activity of the heart to diagnose and/or locate the site of ischemia, infarctions, or other life threatening cardiac events. The likelihood of detecting cardiac ischemia will increase if more EKG leads are used.
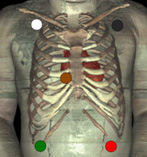
Uses five electrodes (white, green, black, red, and brown)
Gives seven views of the heart
Quick placement reference: Clouds over grass, smoke over fire, brown in the middle
Includes monitor of leads I, II and III (the same angles of the heart as described for 3-lead EKG).
V1 is an additional view of the heart in a 5-lead EKG. It refers to both ventricles and the right atrium. It is an important lead in analyzing ventricular ectopy. V1 can be used to differentiate between the ventricular tachycardia (VT) and supraventricular tachycardia (SVT).
The combination of V1 and Lead II can be used to differentiate between a right or left bundle branch block (RBBB vs. LBBB).
All atrial dysrhythmias, ventricular dysrhythmias, and anterior wall ischemias can be observed and differentiated with a 5-lead EKG; monitoring posterior wall ischemia requires 12 leads.
An additional 6 angles V1-V6 (refer to image for anatomical reference of each lead).
Augmented leads - three additional angles: aVF, aVL and aVR. Combination of these leads with other lead angles allows for diagnosis of ischemic events in a variety of walls.
aVF refers to the inferior wall of the heart.
aVL refers to the lateral wall of the heart
aVR refers to the right ventricle of the of the heart.
References
Barill, T.P. (2003). An ECG Primer Nursecom Educational Technologies. Retrieved on November 4th 2008 at www.nursecom.com/ECGprimer.pdf.
Morton, P.G., Fontaine, D.K., Hudak C.M., & Gallo, B.M. (2005). Critical Care Nursing: A Holistic Approach. (8th ed.). Philadelphia, PA: Lippincott WIlliams & Wilkins.
Urden, L.D., Stacy, K.M., & Lough, M.E. (2006). Thelan's Critical Care Nursing: Diagnosis and Management. (5th ed.). St. Louis, MO: Mosby Elsevier.